


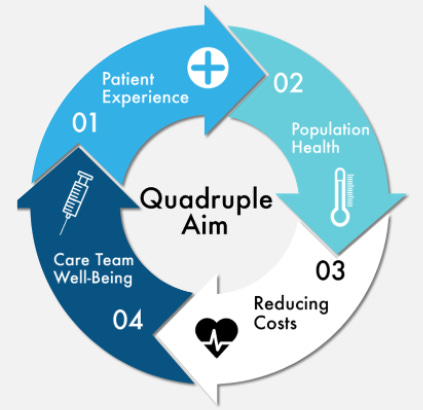
Quadruple Aim

Fifteen years ago, John Whittington and Tom Nolan at the Institute for Healthcare Improvement (IHI) developed a framework for how to think about the goals of healthcare. Before this framework, which they called the Triple Aim, healthcare aims were related to treatment. The Triple Aim added the population goal of health for everyone, including those who were not showing up for treatment. They also added a goal that many of healthcare professionals leave to the administrators—the money. The Triple Aim framework became the standard for thinking about healthcare performance: The best experience of care, the healthiest population, at the lowest cost. Seven years later, doctors Thomas Bodenheimer and Christine Sinsky realized that the Triple Aim was missing an element and proposed the Quadruple Aim. That missing element is the experience of healthcare staff.
The State of Healthcare Interoperability in 2019 - Dimensional Insight (dimins.com)
When the last element of the Quadruple Aim was first proposed, no one could have predicted our workforce situation. Now, more than ever, we are in a situation in which the experience of the healthcare workers at every level must be improved or the rest of the aims are impossible to achieve. This was clear to many in the field long before the Covid-19 pandemic, the great resignation, and the unpredictable economy led to our current workforce crisis. Staff experience and satisfaction in their work has such a significant effect on the experience of the patient.
When I was a crisis clinician doing emergency psychiatric evaluations in the community, and starting to burn out, I knew I wasn’t providing the best care to patients. Good crisis planning requires creativity and optimism and exhaustion robbed me of both. When I couldn’t be solution focused, I took the path of least resistance for patients who were having thoughts of suicide—I hospitalized them. Not only is this poor care but it is expensive care. Most people in a psychiatric crisis are best served in their community and hospitalization should be a resource of last resort. My unhealthy experience as a healthcare worker hindered my ability to support any of the other healthcare aims.
Before I burned out, when I was bringing energy and commitment to work every day, the experience of the patient was my priority. I think most people working in healthcare would agree that this is a driver for them. You’ve probably received some sort of patient satisfaction survey from one of your providers. Those surveys often cover the experience from the front door, including scheduling, convenience of the location, front desk staff friendliness, ambiance of the waiting area, through the care experience. They may ask about the amount of time your provider spent with you. Did you get all your questions answered? Did you understand your treatment plan? Was the issue you presented for resolved? There are other ways that healthcare organizations evaluate the patient experience including clinical outcome measures and quality data.
While the patient experience of treatment and care is the most understandable aim for most people, it is one of the smallest slices of our health. Most of our health is not experienced in a care setting, it’s experienced in our homes, workplaces, and communities. How do we think about the health of a population and not just the treatment of a population? This population health aim encompasses much of what public health is working on including vaccines, smoking cessation campaigns, and other public service announcements related to healthy lifestyle choices. It also looks at social determinants of health—the economic, environmental, and social factors that influence our individual health. What are the circumstances that are leading people to become ill and need treatment to begin with?
Finally, a goal of the healthcare system must be to provide whatever is needed at the lowest cost because like it or not, health costs money and the more efficient we are with our costs, the more people we can help. My first job in Philadelphia was at Community Behavioral Health (CBH), the city’s behavioral health managed care organization. Providers would call me and present a case and their proposed treatment, and I would either approve the service, or pass it along to a physician with a recommendation for denial. This is a gross simplification of what precertification entails. As I would explain my job to family and friends, I often received a grimace or some sort of judgment that my job was to deny healthcare. While I understand that inclination, the truth is that there is a limited amount of Medicaid money. It must be thoughtfully spent, or we end up paying for unnecessary treatment early in the year and having no money to cover essential treatment later in the year. The goal is to provide the exact right treatment—no more, no less.